Olive oil, the gold in the Mediterranean Diet

The Mediterranean diet has proven to have health benefits to the population of the countries that consume it, such as Spain, Italy and Greece. For years researchers have observed lower incidences of certain diseases in the Mediterranean countries. Thus, the Mediterranean diet has been the scope of many research groups in order to understand which elements of this diet protect individuals from a range of diseases, including heart diseases.
One ingredient very valued in the Mediterran diet is olive oil. The beneficial effects of olive oil have been attributed to its content in oleic acid, a monounsaturated fatty acid (MUFA). In addition, olive oilcontains significant amounts of phenolic antioxidants and other phytochemicals (tocopherols, polyphenols). These phytochemicals are especially high in extra virgin olive oil (EVOO) and are present to a lower extent in common refined olive oils.
Since 2003, a large randomized trial in Spain studies the effectiveness of a Mediterranean diet (MeDiet) on the primary prevention of cardiovascular disease (CVD). The study is named “PREvencion con DIeta MEDiterranea” (prevention with Mediterranean Diet), abbreviated as PREDIMED. The main outcome of the study is the incidence on cardiovascular disease.
The study comprises 7,447 participants randomized to three different interventions: a MedDiet supplemented with EVOO, a MedDiet supplemented with mixed nuts, or advice on a low-fat diet (control diet).
The participants of the study did not have CVD at enrolment, but they were at high cardiovascular risk because of the presence of type 2 diabetes or at least three of the following risk factors: current smoking, hypertension, high low/density lipoprotein (LDL), low high-density lipoprotein(HDL), overweight or obesity and family history of premature CVD.
To assess the dietary habits of the participants, trained dieticians completed a 137-item food frequency questionnaire (FFQ) in a face-to-face interview at baseline and yearly during the follow-up. FFQ assess habitual diet by asking about the frequency with which food items are consumed over a period of time. In addition, the participants had to answer a questionnaire designed to assess the adherence to the traditional MedDiet (Table 1).

Several publications have arisen from the PREDIMED study, which confirm that the MedDiet is effective for the primary prevention of CVD in a high-risk population1.
The PREDIMED study is an interventional study of long-term follow-up that provides the opportunity for additional observational cohort studies to take place in high cardiovascular risk subjects in a Mediterranean setting. One of such observational prospective cohort study was carried out by a research group at the Human Nutrition Unit of the University Hospital of Sant Joan de Reus (Spain)2.
In their study, Guasch-Ferre and coworkers divided all participants of the PREDIMED study according to their total intake of olive oil. They obtained the information on olive oil consumption from the FFQ that the participants of the PREDIMED study completed.
The amount of olive oil consumed by the participants was divided depending on the type of oil they were consuming:
– EVOO, produced by mechanically pressing of the olives, acidity <1%
– Common olive oil, composed by:
refined olive oil, acidity <0.3%)
pomace olive oil, obtained from the residues of pressing the olives and mixed with other refined olive oils, acidity <0.3%
The dietitians asked the participants how often they ate olive oil (EVOO or common olive oil) and calculated from the answers the amount of olive oil consumed by the participants in grams per day. Then the participants were divided in three groups according to the amount of olive oil that they consumed. In statistics, these groups are called “tertiles”. Thus, participants were divided in three tertiles:
Tertile 1: low olive oil intake
Tertile 2: medium olive oil intake
Tertile 3: high olive oil intake
During a median of 4.8 years of follow-up, 277 incident cases of major cardiovascular events, 81 cardiovascular deaths, 130 cancer deaths and 323 all-cause deaths occurred. The mean age of the participants was 67 years and 57.4% of them were women.
To assess the association between olive oil intake and risk of CVD, the authors used a multivariate Cox model, a logistic regression analysis that takes into account the time point when certain event occurs. Three different Cox models were used. Model 1 was adjusted for age, sex and the intervention group in the PREDIMED study (MedDiet with EVOO, nuts or low fat diet). Model 2 was additionally adjusted for body mass index (BMI, kg/m2), smoking status, alcohol intake, educational level, leisure time physical activity, prevalence of diabetes, prevalence of hypertension, prevalence of hypercholesterolemia, use of antihypertensive medication and use of statins. Model 3 was adjusted for adherence to the MedDiet.
The findings for the association of CVD risk and total olive oil intake are summarized in Table 2. The results are expressed as hazard ratios (HRs) with 95% confidence intervals (CIs). In clinical trials, the HR is an expression of the chance of events occurring in the treatment arm (here tertile 2 and 3) as a ratio of the chance of the events occurring in the reference arm (in this study tertile 1).
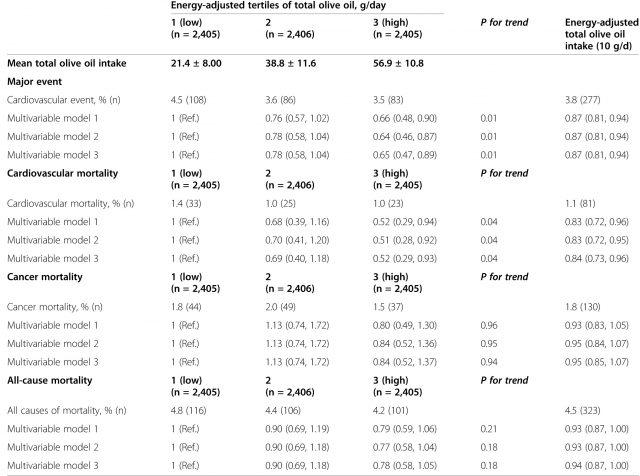
The authors observed up to 36% lower risk of major cardiovascular event and 42% lower risk of cardiovascular death among individuals in tertile 3 of total olive oil intake as compared to those in tertile 1.
In addition, the authors also analyzed the consumption of olive oil as a continuous variable, i.e., what is the effect of consuming certain amount of olive oil across all the participants. With this analysis they observed that for each 10 grams/day (one tablespoon) of olive oil the risk of a major cardiovascular event decreased by 13% and the risk of cardiovascular mortality decreasedby 16%. In Table 2 this result is expressed as “energy adjusted total olive intake (10 g/day)”.
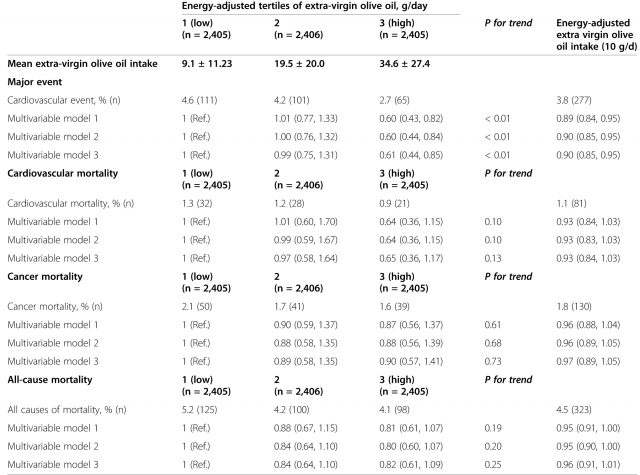
Next, the authors analyzed the risk of CVD according to the type of olive oil participants consumed, i.e., EVOO or common olive oil. For EVOO, there was a 40% lower risk of major cardiovascular event and a 35% lower risk of cardiovascular death among individuals in tertile 3 as compared to those in tertile 1 (Table 3). On the other hand, for common olive oil no reduction on the risk of major cardiovascular event was observed and the reduction of cardiovascular death was only of 19% (Table 4).

No statistically significant associations were found for olive oil consumption and cancer mortality and all-cause mortality.
The results from this observational study confirm the importance of olive oil consumption in the Mediterrean diet. Although other components of the Mediterranean diet such as nuts, vegetables, fruits, legumes and fish might play together to produce the observed cardio-protective effects, it is clear that olive oil, in particular EVOO, has a pivotal role protecting the Mediterranean population from CVD.
In conclusion, the present study proves that greater consumption of total olive oil, especially EVOO, is associated with reduced cardiovascular disease and mortality risk in an elderly Mediterranean population at high cardiovascular risk. The results of this study point out olive oil consumption as one of the key components of the Mediterranean diet for cardiovascular disease prevention. Thus, according to this study, there is nothing wrong making your salads tastier with some extra olive oil. Enjoy it!
References
- Martínez-González MÁ, Corella D, Salas-Salvadó J, Ros E, Covas MI, Fiol M, Wärnberg J, Arós F, Ruíz-Gutiérrez V, Lamuela-Raventós RM, Lapetra J, Muñoz MÁ, Martínez JA, Sáez G, Serra-Majem L, Pintó X, Mitjavila MT, Tur JA, Portillo MP, Estruch R; PREDIMED Study Investigators. Cohort profile: design and methods of the PREDIMED study. Int J Epidemiol. 2012, 41(2):377-85. ↩
- Guasch-Ferré M., Miguel A Martínez-González, Montserrat Fitó, Mònica Bulló, Ramon Estruch, Emilio Ros, Dolores Corella, Javier Recondo, Enrique Gómez-Gracia & Miquel Fiol & (2014). Olive oil intake and risk of cardiovascular disease and mortality in the PREDIMED Study, BMC Medicine, 12 (1) 78. DOI: http://dx.doi.org/10.1186/1741-7015-12-78 ↩
3 comments
[…] Denok entzun dugu zer nolako onurak dituen dieta mediterraneoak gure osasunean. Hala ere, orain hasi gara ezagutzen benetan zer duen dieta horrek hain onuragarria izateko. Onura dakarren elementuetariko bat da oliba olioa (hobe olio birjina). Laura Cascalesek kontatzen digu: […]
[…] Todos hemos oído hablar de las ventajas para nuestra salud de la dieta mediterránea. A pesar de ello solo ahora empieza a conocerse qué es lo que tiene en concreto que la haga beneficiosa. Y una de esas cosas […]
[…] Image source […]