“…the proper application of Darwinian thinking to human issues- of mind, language, knowledge, and ethics, for instance- illuminates them in ways that have always eluded the traditional approaches, recasting ancient problems and pointing to their solution.”
Darwin’s Dangerous Idea, by Daniel Dennett, 1995
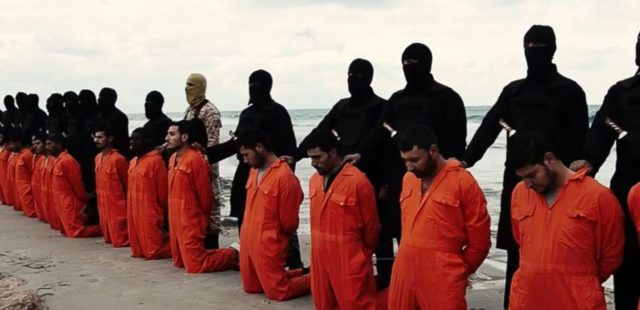
This series of articles will discuss killing – homicides, assassinations, wars and executions – from a biological, evolutionary standpoint. As a preamble, I would like to remind the reader – at the same time that I remind myself as the writer – that the culture, history and ideology of both the reader and the writer have an impact on the interpretation of hypotheses and theories – and even on which facts are chosen to be taken into account. In the case of this series of articles, above all I will strive to be mindful of how my personal circumstances have an impact on these reflections.
In the film Anzio, Robert Mitchum plays the protagonist, a cynical war veteran and journalist. Towards the end of the film, speaking to a decommissioned general, Mitchum’s character states “…men kill because they like it”. This is followed by several (not altogether cogent) explanations of his assertion. I have always been fascinated by the fact that, even as we emphasize minding the fifth commandment, thou shalt not kill, we kill all the time. The Bible clarifies in Exodus 23:7, “…do not kill the innocent and righteous. For I will not justify the wicked”, making a more precise point about when we must kill and when not.
As I write these lines, people are suffering violent death in many parts of the world, whether their inhabitants deem their world as civilized or not. Humans kill and have killed each other in all cultures, places and times. The question is why we do it.
In the United States there were 13,636 homicides in 2009. Nearly 88 million people died as a result of the wars of the twentieth century, 54 million of whom were civilians. Amongst hunter-gatherer tribes, whose way of life is closer to that of all humans thousands of years ago, 13 % of men (according to archeologists) or 15 % (according to current ethnography) perish in war. Amongst the Yanomamo of the Amazon, 20 to 30 % of men die violently.
These are just some of the statistics that illustrate the magnitude of violence that our species inflicts upon itself. We may add that, although some of these deaths may be have been to mental disorders, alcohol, drugs or similar factors, most cases of violent behavior in our species are not aberrations, but the behavior of ordinary people. Wars and homicides are habitual, typical human behavior.
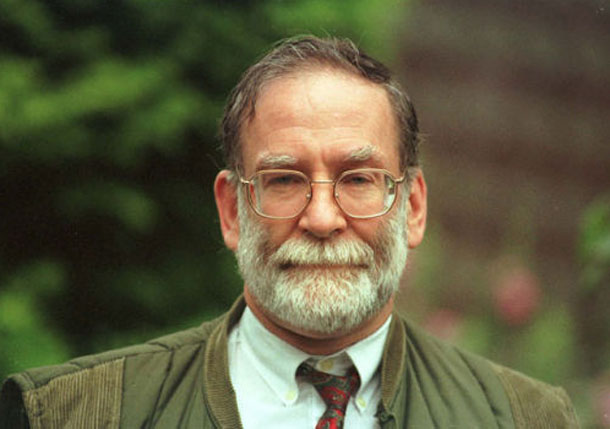
The ambitious physician, Harold Shipman, and how statistics belatedly shed light on his crimes
Portrait of Harold Shipman
The story of Harold Frederick Shipman, an English general practitioner who near the end of his life became known as a serial killer, is the first of several case studies in this series that aim to illustrate the human capacity for killing. Although Dr. Shipman’s case is extreme, it is an example of how a well-respected, apparently ordinary man was capable of an enormity of crimes. Suspected of the murder of hundreds, he was convicted to fifteen consecutive life sentences for the murder of fifteen of his latter victims. He committed suicide in 2004 confined to his cell in Wakefield prison. He never admitted guilt, did not divulge how many people he had killed, nor what were his motives for having done so.
Dr. Shipman was born in Nottingham in 1946, where he went to medical school, later studying at the University of Leeds. He became a resident physician at Bodington Hall Faculty of Medicine, where he met his future wife, Primrose May Oxotoby. They married in 1966 and had four children. After finishing his medical education, Dr. Shipman began to practice medicine at Pontefract Hospital near Leeds (where some suspect his killing began) and later worked in penitentiary settings, where, again, it is suspected that he killed several patients.
Early signs of trouble surfaced in 1975, when, denounced by colleagues, he was censured and fined for forging pethidine prescriptions for his personal use (pethidine, or Demerol, is a synthetic opioid considered to be less addicting than morphine). After completing a program at a detox center, he was declared fit to resume practicing medicine.
In 1985, Allen Massey, the undertaker at a local funeral home, confronted Dr Shipman with unusual features of his practice and with the peculiar circumstances of his patient’s deaths. Firstly, Dr Shipman had a greater proportion of patients die than one would expect. Many of them died while fully dressed, sitting on their couch at home. Many had not been considered gravely ill before their death. Moreover, Dr. Shipman seemed to be very often present at the time of death. But Dr. Shipman, offering his medical records for inspection, managed to convince Massey that there was nothing untoward.
Shipman moved from one position to the next, always leaving a favorable impression, and finally ended up in Hyde, near Manchester, where he established his own private clinic in 1993. Suspicion then rose again, just across the street from his clinic, where physicians from the Brooke Clinic remarked on the excess of deaths in Shipman’s practice. But again, proving wrongdoing was difficult.
He finally came under sustained legal suspicion for serious misdeeds in 1998. It started when Doctor Linda Reynolds expressed concern to the South Manchester coroner, John Pollard. Dr. Reynolds had noticed that Shipman’s patients suffered an unusually high mortality, that patients who died while under his care were cremated more frequently than usual, and that most of them – up to 80% – were older women. Pollard agreed that Shipman seemed to be killing his patients, although he could not say whether this was due to negligence, or murder. The police conducted a perfunctory investigation, and the case was closed after one month, due to lack of evidence.
It was the death of his last victim, Kathleen Grundy, that re-opened his case later that year. Ms. Grundy was a well-known personality, having been at one time the mayor of Hyde. She had received a home visit from Dr Shipman on the day of her death at the age of 81. Dr. Shipman, signing her death certificate, certified the cause of death as “ old age.”
Ms. Grundy’s daughter, Angela Woodruff, a lawyer, soon learned that her mother had changed her will, leaving her savings to Dr. Shipman. The will document was sloppily typed and poorly redacted. Ms. Grundy had not owned a typewriter. Ms. Woodruff turned to the police and managed to arrange for the exhumation of her mother’s cadaver. Analysis revealed an overdose of morphine, apparently administered about three hours before her death – a time that coincided with Shipman’s visit. He was arrested on September 7, 1998. The typewriter that had been used to forge Ms. Grundy’s will was found in his home.
The police then centered their investigation on the last 15 patients who had died while under Shipman’s care. All 15 had traces of morphine in their remains. With this information at hand, Dr Shipman was charged, and in October 1999 his trial commenced. A policeman who had questioned Shipman testified that he was a difficult, arrogant man, who tried to control the interrogations and mocked the police, taking the process a contest where his superior intellect would surely emerge victorious. But Shipman was found guilty and sentenced to 15 consecutive life sentences, one for each of his known, latter victims. The judge added a recommendation that he never be paroled. Shipman never confessed any culpability. On January 13, 2004, one day before his 58th birthday, he committed suicide in his cell.
Shipman had been very close to his mother, who had died at the age of 43, when Shipman was only 17. In some ways his mother had passed away as his victims would in years to come: She died at home, where her physician had been administering morphine for cancer pain. Most of Shipman’s murders would follow a similar pattern: During a home visit some weekday afternoon, morphine or heroin would be administered, but this time in overdoses meant to kill. The patient would be found dead shortly after the doctor had left – or sometimes would expire while he was present. The cause of death would be certified as a heart attack, a stroke, or simply, old age. The family of the decedent accepted that the death was due to natural causes, and, upon the recommendation of the physician, often had the body cremated.
After Shipman’s suicide a British governmental investigation, presided by judge Janet Smith, estimated that Shipman had murdered some 250 of the 454 patients who had died while under his care. The report concluded with recommendation to restructure the practice of medicine, based upon the troubling aspects of Dr. Shipman’s record that should not have been overlooked, such as the excessive use of morphine, a pattern of home visits shortly before the death of patients, a disproportionate percentage of elderly women amongst the decedent, a disproportionate percentage of cremations, etc. The report also made recommendations to address systemic issues such as the risks of solo medical practices, improving official response to complaints regarding physicians, updating the role of forensic specialists, etc. It was clear that many protocols regulating medical practice in Great Britain had to be revised – remarkably, a salutary review prompted by the crimes of a serial killer.
Statistical studies followed that shed further light on the case by comparing Dr. Shipman’s record with those of other physicians. Richard Baker, of the University of Leicester, conducted a study upon the recommendations of a medical council, regarding the pattern of deaths certified by Dr Shipman in his 24 years of practice. Shipman certified nine times more death certificates that other doctors in his locality and listed the cause of death as “old age” eight times as frequently. Most of his patients died between 2 PM and 4 PM, whereas the patients of other doctors died at random times during the day. The family members of other doctor’s patients were present at the time of death in about 80% of the cases, but only in about 40% of Dr Shipman’s. His patients died rapidly, 60% within half an hour, while only 23% of other physician’s patients died so quickly. Dr Shipman was recorded as being present during the death of 19 % of his patients, while less than 1% of other doctors were. Overall, if Dr. Shipman was the physician of record, the risk of sudden death surpassed the risk of sudden death associated with smoking. Richard Baker concluded that Shipman had killed 236 patients.
For reasons unknown, the medical profession, closely followed by nursing and to a lesser degree dentistry, is marred by the greatest number of serial killers amongst its practitioners (mere access to lethal means is not a sufficient explanation – for example, veterinary medicine does not carry this peculiar taint). One must exercise caution in getting medical care!
Regarding the use of statistics, we can see that even applying its methods, it is not easy to detect a medical serial killer. If one only considers the overall numbers, a red flag may not stand out: Shipman had about 3000 patients concurrently, so the death of 15 to 20 of them during his latter career may not have reached statistical significance. Remarkably, it took the forgery of Kathleen Grundy’s will to give him away.
Not having any personal experience in killing, it has been my intellectual formation and interest that have led me to apply concepts of evolutionary biology and psychology to examine what mental functions are manifested in violence that can lead to killing. Very generally, the principal hypothesis is that violent behavior served individuals in ancestral environments to gain resources to reproduce. A tendency to violence could then become a selective advantage in the evolutionary process. And thus, as an evolutionary advantage, it has reached us in our day and age.
The two reproductive objectives that our ancestors pursued, and that we continue to pursue, are survival and reproduction proper. Firstly, survival is necessary to reproduce, and for survival food, shelter and a safe enough environment are needed. As such, many conflicts within groups and between groups were due to the scarcity of resources needed for survival. Let us remember a scene from the first part of 2001, A Space Odyssey, by Stanley Kubrick, to get a sense of this struggle – depicting, in the case of the film, the struggle for food and water.
Scene from 2001, A Space Odyssey
The second objective is obtaining a mate, which is the primary resource for reproduction. Depending on circumstances, the means that facilitate obtaining a mate may differ. For example, controlling territory rich in resources, having allies that can aid in defense, enjoying high social status, possessing weapons, or goods that require manufacture, such as clothing, precious objects, adornments, accessories, etc. In recent centuries, we may add, possessing money – which may not buy happiness, but certainly helps to secure resources needed for evolutionary success. Some of these resources may not further survival per se, nor the procuring of mates, but instead create the capacity to inspire fear and respect. This is the payoff of having weapons and high status. Consequently, men in competition are more prone to violence than women. What is more, those same features may, in turn, become attractive to women, because they themselves may have been selected to choose men whose proneness to competitive violence procures children with more resources.
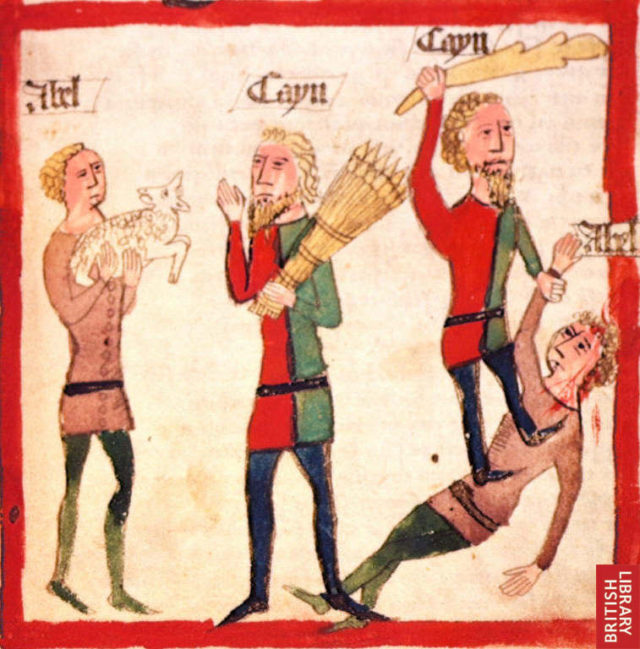
Cain and his brother Abel
Cain and Abel from “Speculum Humanae Salvationis”
Murder makes its appearance very early in the Bible – witness the drama of Cain and Abel, which unfolds just barely after the story of humankind begins:
Genesis 4: 2-14; King James Version
And she again bare his brother Abel. And Abel was a keeper of sheep, but Cain was a tiller of the ground. And in process of time it came to pass, that Cain brought of the fruit of the ground an offering unto the LORD. And Abel, he also brought of the firstlings of his flock and of the fat thereof. And the LORD had respect unto Abel and to his offering: But unto Cain and to his offering he had not respect. And Cain was very wroth, and his countenance fell.
And the LORD said unto Cain, Why art thou wroth? and why is thy countenance fallen? If thou doest well, shalt thou not be accepted? and if thou doest not well, sin lieth at the door. And unto thee shall be his desire, and thou shalt rule over him.
And Cain talked with Abel his brother: and it came to pass, when they were in the field, that Cain rose up against Abel his brother, and slew him.
And the LORD said unto Cain, Where is Abel thy brother? And he said, I know not: Am I my brother’s keeper?
In very general terms then, a propensity to violence has been selected because it leads to obtaining resources and achieving reproduction. Such violence has been mostly that of young men against each other. But also, if women find dominant and aggressive men (consequently, resource-rich men) attractive, this would suggest that, ultimately, both sexes have contributed to the evolution of violence in our species.
The difference between the sexes in relation to violence relates to the difference in the behavioral objectives tied to reproduction. Men compete with other men for sexual access to as many women as possible, aiming to bequeath more of their genes to subsequent generations. But men must also dedicate resources to their mates during her pregnancy, during the early care and breastfeeding of infants, and generally, to the development of their children. Thus, men’s objectives are twofold – obtaining more mates, but also ensuring that their offspring, which carry their genes, are successful.
Women, on the other hand, do not waste their resources in disputing access to more men. Rather they dedicate effort in finding a mate with good reproductive value, that is, a young and healthy man, that can contribute with his resources to the care and growth of their children. Men tend to seek short term mating, while women seek longer term mating that includes the goal of caring for children in the longer term.
All this being said, we must remember that the environment in which our ancestors lived was very different from the one humanity shares today. Thus, the selective forces that acted upon on tendencies to violence may not operate today. Killing in our culture is not defensible except in very specific situations. Still, we should not forget that sanctioned killing remains – we still have armies and, in many countries, still have the death penalty.
One of the most violent behaviors typical of our species is war, that is, violent confrontations between human groups, confrontations that one could call “official”. Human groups make war possible. But in order for groups to have arisen, cooperative, empathic relationships between individuals was necessary. Without prior cooperation, there could be no subsequent war – at most, there would have been only combat between individuals. As we can see, tendencies to both violence and to cooperation, selected by the evolutionary process, are flip sides of the same behavioral tendencies of our species. Perhaps the only way to control and even end interpersonal violence will be by the fostering and development of cooperative, empathic and altruistic behaviors.
Finally, debating which tendencies toward violent behavior are biological adaptations and which are not, I propose that all acts of violence are rooted in an evolutionary history related to resource acquisition. But then, as happens with other evolutionary processes, tendencies towards violence which were selected for one purpose may be selected and recombined anew for other purposes.
References:
Baker, R., D.R. Jones & P. Goldblatt. 2003. Monitoring mortality rates in general practice after Shipman. British Medical Journal 326: 274-276.
Baumeister, R.F. 2001. Raíces de la violencia. Investigación y Ciencia junio.
Buss, D.M. 2005. The murdered next door: Why the mind is designed to kill. Penguin Books. New York. 288 pp.
Buss, D.M. 2012. The evolutionary psychology of crime. Journal of Theoretical and Philosophical Criminology Special Edition January: 90-98.
Buss, D.M. 2013. The science of human mating strategies: An historical perspective. Psychological Inquiry 24: 171-177.
Duntley, J.D. & D.M. Buss. 2004. The plausability of adaptations for homicide. En “The structure of the innate mind”. Ed. por P. Carruthers, S. Laurence & S. Stich. Oxford University Press. New York.
Ferguson, R.B. 2003. The birth of war. Natural History July/August: 27-35.
Frankel, S., J. Sterne & G.D. Smith. 2000. Mortality variations as a measure of general practitioner performance: implications of the Shipman case. British Medical Journal 320: 489.
García, J.E. 2015. El comportamiento criminal desde un punto evolucionista. Persona 18: 27-46.
Guthrie, B., T. Love, R. Kaye, M. MacLeod & J. Chalmers. 2008. Routiny mortality monitoring for detecting mass murder in UK general practice: test of effectiveness using modelling. British Journal of General Practice May: 311-317.
Jackson, T. & R. Smith. 2004. Obituaries: Harold Shipman. A general practitioner and murderer. British Medical Journal 328: 231.
Kinnell, H.G. 2000. Serial homicide by doctors: Shipman in perspective. British Medical Journal 321: 1594-1597.
Liddle, J.R., T.K. Shackelford & V.A. Weekes-Shackelford. 2012. Why can’t we all just get along? Evolutionary perspectives on violence, homicide, and war. Review of General Psychology 16: 24-36.
Morrall, P. 2006. Murder and society. John Wiley & Sons. Chichester. 214 pp.
Pringue, M. 2000. The Shipman inquiry: implications for the public’s trust in doctors. British Journal of General Practice May: 355-356.
Winter, D.A. 2016. Construing homicide. En “The Wiley handbook of personal construct psychology”, p. 416-425. Ed. Por D.A. Winter & N. Reed. John Wiley & Sons. New York.
1 comment
[…] 2017an Eduardo Angulok Cuaderno de Cultura Científica -n “Preparados para matar” (Hiltzeko prestatuak) artikulu sorta idatzi zuen, non espeziearen jokaera bortitza analizatzen zuen. Julio Ozores psikiatraren eskutik ingelesezko bertsio moldatua dugu: Prepared to kill: Some ideas to debate. […]


1 comment
[…] 2017an Eduardo Angulok Cuaderno de Cultura Científica -n “Preparados para matar” (Hiltzeko prestatuak) artikulu sorta idatzi zuen, non espeziearen jokaera bortitza analizatzen zuen. Julio Ozores psikiatraren eskutik ingelesezko bertsio moldatua dugu: Prepared to kill: Some ideas to debate. […]