Bilingual brain surgery
The number of people who speak one language (monolinguals) is rather small today1 , with many of us growing up with more than one language or learning another one during our lifetime. Language experts argue that what counts as speaking two languages (bilingualism) is not only a matter of the number of languages we speak, but also of their usage, proficiency, and even of the similarity between languages2. Bilingual speakers are lucky today, as research shows that they may present delayed cognitive deterioration when affected with dementia3 they can be faster at switching between tasks4, and even have higher grey matter density in specific brain areas!5People who speak more than one language, however, may have to go through specific procedures when undergoing brain surgery, due to particularities of brain structures responsible for language processing.
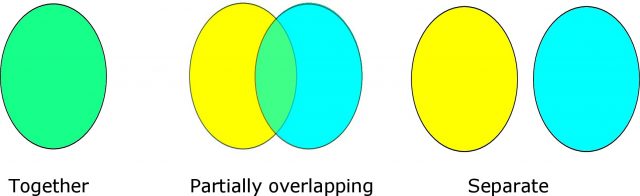
In 1867, Robert Scoresby-Jackson asked the scientific community whether different languages may be processed in different brain regions6. There are essentially three views for the representation of two languages in the brain: (1) two languages processed together in the same areas, (2) a partial overlap between languages in the same areas, or (3) two languages produced in separate brain areas. A definite answer does not exist as of today, which raises the question of whether or not a bilingual person who undergoes surgery may suffer language impairment in one language but not in another, or whether, during surgery, it may be possible to find brain areas that are related to language processing in language A but not in language B. A procedure called awake surgery provides some insights into this issue.
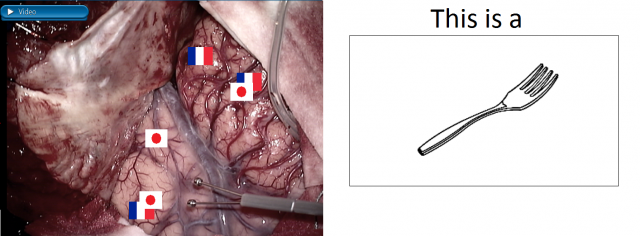
In 1978, George Ojemann and Harry Whitaker7 applied weak electrical currents to the brain of people who were undergoing brain surgery and, at the same time, asked them to name pictures of objects. This approach is called “awake surgery” and the idea behind it is to be able to stop the responses of patients during stimulation of specific brain sites. When this happens in at least two of three trials, it is thought that the area (or brain network) where electrical stimulation was delivered is responsible for language processing. Hence, the area or areas where this phenomenon happens are left untouched during the removal of a tumour or epileptic foci, as removing those areas may increase the risk for language deficits after surgery.
The beauty of the work by Ojemann and Whitaker was that they went a step further from what had been done up until then, and asked patients not only to name pictures but to do so in the two languages they were able to use. The findings of these authors were quite revealing: they reported brain areas where it was possible to stop the responses of patients while they were saying the names of pictures in two languages, and specific areas where it was only possible to stop the responses of the patients when they were responding in one language, but not in the other. This is quite an enlightening finding for three reasons: it indicates that it is possible to ask people to say the names of pictures in two different languages during surgery, that there may be areas of the brain that respond to one language but not another one and vice versa, and it points to the fact that the representation of language in the brain may partially overlap!
After this pioneering work, more and more groups have become interested in this procedure. In 2007, Carlo Giussani and colleagues8 reviewed the work of 7 different surgical groups who, all together, had operated on 88 bilingual people. Six of the groups asked patients to name of objects when seeing pictures (i.e., object naming). From the same groups, two others combined a reading task with object naming, and one group used a reading task. Similarly to the initial study by Ojemann and Whitaker7, all surgical groups found brain areas where it was possible to stop the responses of patients with two languages, but also areas where it was possible to stop the responses of patients when the patient was responding in one of the two languages.
Using tasks in more than one language may help to avoid language damage in people that undergo such surgical procedures, and help answer relevant theoretical questions about the relation between the brain and language910. Of course, evidence from brain surgery alone is not enough to answer a question such as that posed by Scoresby-Jackson, particularly today when it is possible to also scrutinize data from other lesion studies as well as those from neuroimaging techniques5. However, to the extent that different areas may be encountered using tasks in different languages, it seems that providing bilinguals with tasks in their two languages may help to avoid language damage. To put it short: marrying neurosurgery with Cognitive Neuroscience brings a direct benefit to brain health and, at the same time, a careful look at the research data provides an excellent window to understand how language is processed in the brain.
References
- Tucker, G. R. (1999). A global perspective on bilingualism and bilingual education. In J. E. Alatis & A. Tan (Eds.), Georgetown University Round Table on Languages and Linguistics (332-340). Georgetown: Georgetown University Press. ↩
- Ardila, A. (1998). Bilingualism: A neglected and chaotic area. Aphasiology,12(2), 131-134. ↩
- Bialystok, E., Craik, F. I., & Freedman, M. (2007). Bilingualism as a protection against the onset of symptoms of dementia. Neuropsychologia,45, 459-464. ↩
- Prior, A., & MacWhinney, B. (2010). A bilingual advantage in task switching. Bilingualism: Language and cognition, 13, 253-262 ↩
- Mechelli, A., Crinion, J. T., Noppeney, U., O’Doherty, J., Ashburner, J., Frackowiak, R. S., & Price, C. J. (2004). Neurolinguistics: structural plasticity in the bilingual brain. Nature, 431, 757-757. ↩
- Scoresby-Jackson, R. E. (1867). Case of aphasia with right hemiplegia. Edinburgh Medical Journal, 12, 696-706. ↩
- Ojemann, G. A., & Whitaker, H. A. (1978). The bilingual brain. Archives of neurology, 35, 409-412. ↩
- Giussani, C., Roux, F. E., Lubrano, V., Gaini, S. M., & Bello, L. (2007). Review of language organisation in bilingual patients: what can we learn from direct brain mapping?. Acta Neurochirurgica, 149, 1109-1116. ↩
- Rofes, A., & Miceli, G. (2014). Language mapping with verbs and sentences in awake surgery: A Review, Neuropsychology Review, 24, 185-99. ↩
- Goral, M., Levy, E. S., & Obler, L. K. (2002). Neurolinguistic aspects of bilingualism. International Journal of Bilingualism, 6, 411-440. ↩